|
|
|
When the amount of tissue (skin) that is required to be removed cannot be simply sutured(stitched) together, repair with skin imported from elsewhere on the patient is required. Flap repairs use immediately adjacent skin which is moved into the defect whilst maintaining a blood supply to that flap. Alternately, skin grafts can be harvested from distant sites (eg around the ear or neck) and secured into the tumour excision defect. These grafts have to develop a new blood supply from the base and edges of the defect into which they are placed. |
|||||||||||||||||||||||||||||||||||||||||||||||
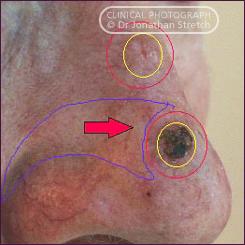
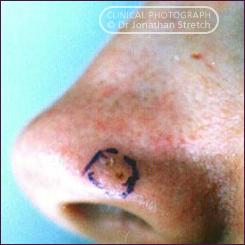
BCC
of the nose and graft repair |
|||||||||||||||||||||||||||||||||||||||||||||||
 |
 |
||||||||||||||||||||||||||||||||||||||||||||||
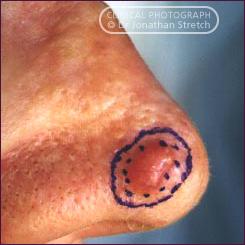
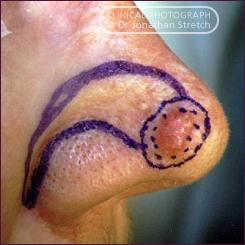
| This patient had a recurrent Basal Cell carcinoma on the nostril margin. |
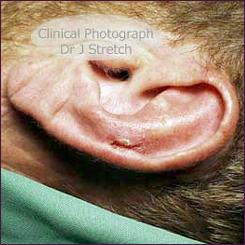
The defect was repaired with a skin graft taken from an inconspicuous donor site in front of the ear where a close match of skin colour and texture was available.Result after 12 months.
|
||||||||||||||||||||||||||||||||||||||||||||||
|
Jonathan
Stretch Plastic Surgeon D.Phil (Oxon) F.R.A.C.S.
|
|||||||||||||||||||||||||||||||||||||||||||||||




 An
island of skin with attached blood vessels is raised from
a donor area behind the ear and transfered through a window
in the cartilage.
An
island of skin with attached blood vessels is raised from
a donor area behind the ear and transfered through a window
in the cartilage.